“Every tooth in a man’s head is more valuable than a diamond.”
-Miguel deCervantes
The twenty-first century has provided society with some of its greatest advancements. Beyond cellphones, self-driving cars, and the like, advancement within the world of medicine is progressing at a breakneck pace. While all this achievement has made us stronger and healthier than ever before, there are two major issues that have arisen because of it. First is that medical professionals today get so caught up in science and five-syllable words that they forget to take the time to simplify and break down these large concepts into information that can be understood by someone who hasn’t studied it for eight years. Second, people seem to be so bombarded with (sometimes conflicting) information about their overall health that they forget to pay attention to the very basics of personal health. The aim of this blog is to combat both of these issues as they pertain to oral health by offering basic and understandable information about dentistry and to explain it with more depth than your general dentist may have time to at your next appointment. This way, dentistry may finally receive some much-needed spotlight and readers can confidently take better control of their oral health. Welcome!
Throughout these past weeks, we have covered a very small fraction of the large and diverse aspects of dentistry and oral health. So the question stands here on this final week: why does any of it matter? Why should anyone care about teeth past their ability to chew and their aesthetic qualities? Most people don’t know the extent to which dental hygiene affects overall health. The aim of today’s post is to help make some of those connections more clear.
The Heart of the Issue: Connections with the Cardiovascular System
On the blog, we have discussed at length the effects of plaque in the mouth, but it exists elsewhere in the body. In this article by the Mayo Clinic, oral health is likened to “a window to your overall health.” They go into further detail, calling attention to a condition called endocarditis. Like we’ve done before, let’s break down the Latin: “endo-” means inner or inside, “card” refers to the heart, and “-itis,” as we’ve discussed, means inflammation. So, endocarditis is an inflammation of the inner tissues of the heart. In severe cases, this condition can be detrimental to the function of the heart. It occurs when bacteria from other parts of the body enter the bloodstream and infiltrate the chambers of the heart. As one of the regions of your body with the most diverse bacterial flora, it is incredibly common that this bacterial originates in the mouth.
Oral bacteria also have adverse effects on blood vessels. Back to plaque! Indeed, this runty refuse can be found in the blood vessels, also! Once oral bacteria and their waste enter the bloodstream, the plaque can stick to the artery wall and to itself, narrowing or even cutting off the blood flow in a specific area. At best, this can contribute to high blood pressure. At worst, it can cause cardiovascular disease or even stroke. Especially for those with a family history of cardiovascular issues, dental health should be a top priority.
A Breath of… Air: Connections with the Pulmonary System
Medical professionals really like coming up with arbitrary scientific names, don’t they? The pulmonary system is what we use to refer to the lungs and the pathway thereto. Here, there is one major concern. Normally, our pulmonary system is wired to begin with air entering via the nose. The nose is equipped with a built-in filtration system (unless you pluck it out) which also acts as a humidifier for air entering the lungs. However, evolution has given us the option to breathe through our mouths. This is not optimal, but is extremely common, especially when we sleep. Poor oral hygiene, complete with food particles, bacteria, and plaque, can lead to a slew of issues with the lungs, most notably pneumonia. So, if the idea of having bacteria poo all over your teeth doesn’t make you want to scrub them, perhaps the thought of pneumonia will!
“New” Research: Connections with Alzheimer’s
It’s no secret that Alzheimer’s disease is an incredibly serious condition. Patients with Alzheimer’s begin to lose memory and brain function as their brain begins to deteriorate. A “new” study (I use quotation marks because the study is from 2013, but in the scope of medical history, that is the blink of an eye) from the University of Central Lancashire found P. gingivalis in the brains of dementia patients consistently. This strain of bacteria, as the name suggests, is most commonly found in the mouth. They theorize that the bacteria enters the blood stream during invasive dental procedures and works its way to the brain, triggering an immune response which may damage certain parts of the brain. While this research is not confirmed, other sources also have similar theories.
In Conclusion: Take Care of Your Teeth
This very short list is just a mere glimpse of how your oral health affects the rest of your body. In fact, this blog has only covered a tiny fraction of the massive field of dental science. People spend their lives studying this information and their theories. What do you need to take away? The same things you’ve been told all your life. Brush your teeth twice a day, floss once a day, quit smoking if you do, limit acidic foods and beverage, and visit your dentist once every six months. A dentist told me that the worst and most expensive thing you can do to your teeth is ignore them.
So, dear reader, I implore you to heed my warning and that of millions of dentists before me. Maintaining your oral health takes next to no effort, but is absolutely mandatory for leading a long, happy, and comfortable life. Nobody enjoys getting a root canal, a filling, or even a simple routine cleaning, but trusting your dentist and making their recommendations a priority is imperative. Some people fear that they will be judged for having avoided the dentist for years. While this sort of anxiety is understandable, any respectable dentist will just be glad to work with you from where you are.
I hope this blog has helped clarify some of the abstract concepts within dentistry. If even one person begins paying closer attention to their oral health, I would consider this a success. Besides that, thanks for reading and happy brushing!
That’s right! It’s time for everyone’s favorite: the root canal. When I began shadowing dentists, I thought the root canal was going to be the procedure that finally made me uncomfortable enough to question my career choice. On the contrary, root canals are probably my favorite procedure to watch. To be absolutely honest, root canals and extractions share a lot of similarities. Nobody wants a root canal. They get a bad rap for being painful. Similarly to the extraction, I really can’t offer much in the way of consolation. However, learning about the procedure and its importance may serve to ease some of your anxiety if you have a root canal coming up.
Digging Deeper: What is a Root Canal?
Another thing that extractions and root canals have in common is that they are usually saved as last-ditch efforts to save a tooth. In most cases, if a root canal is to be performed, an extraction has at least been considered. However, root canals are considered preferable, as they maintain much more original tooth structure and don’t leave a gap in your teeth. Gaps in teeth allow things to move around such that additional problems may arise in the future. Although more expensive, root canals are often the preferred course of action for this reason.
“Root Canal” is only the most common name. The procedure is also called “pulpotomy” or “endo” in office shorthand. Dentists who choose to continue their education and specialize in performing root canals are called endodontists, which is where the office shorthand originates. However, my favorite of its names is pulpotomy, as it describes the procedure right in the name (-otomy refers to cutting or removal in Latin, so “pulp removal”). If you need a root canal, your dentist, or endodontist if your case is particularly tricky, will do just that; they will open the tooth and remove the pulp from the crown and root.
Why Me: Why You Need a Root Canal
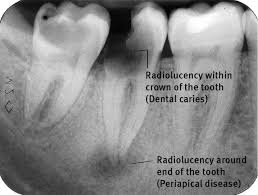
As we’ve already discussed, root canals are not the first line of defense for dental care. In fact, they are among the last measures possible before extraction. There are a number of reasons a root canal may be necessary, but in short, the pulp of your tooth has become infected or damaged in some way beyond what can be fixed with medication. The most common causes are an untreated cavity which has reached the pulp, an abscess beneath the root, or some sort of dental trauma. It just so happens that these are listed from the most to the least preventable.
Obviously, you can prevent an untreated cavity by (wait for it) treating your cavities! All joking aside, proper dental hygiene and regular cleanings and checkups will prevent most, if not all, of this kind of root canal. If left untreated, the acids from the plaque within a cavity will continue to degrade the enamel and dentin until it reaches the pulp, resulting in excruciating pain due to the extensive network of nerves within it. I’ve said it a million times, but believe me. You definitely want to keep up with the brushing and flossing!
Second, and perhaps most common, is the periapical abscess, shown in the x-ray above. Time for more Latin! “Peri-” means “around,” “apical” refers to the apex of the tooth root, and an abscess is a wonderful little pocket filled with a concoction of bacteria, waste, and dead cells. It is somewhat sufficient to think of a periapical abscess as a pimple at the base of your tooth’s root, except it’s in your bone instead of your skin. This apical acne is much more serious, however. Benzoyl peroxide won’t be getting you out of this one in time for senior prom, I’m afraid. As you can see above, these abscesses show up as dark, or radiolucent, meaning they are degrading bone tissue. While it is possible to diminish a small abscess with antibiotics, a pulpotomy is the most effective way of clearing out this infection. Abscess is most common in patients who clench their teeth, or in teeth which have already had some sort of work done.
Finally, dental trauma can also be cause for a pulpotomy. I once saw a man who had gotten headbutted straight in the chin during a local basketball tournament over a decade earlier. His teeth luckily did not all fall out, so he assumed all was well. He now has root canals in all of his mandibular incisors in his mid twenties. Essentially, the other kid’s head acted as the grim reaper himself, for once the collision happened, the teeth were considered “dead.” One way or another, the nerves and blood vessels within his teeth had been cut off, essentially killing the tissue. Dead tissue is perhaps bacteria’s favorite food, so a pulpotomy is often performed to prevent an abscess.
Route to the Root: The Procedure
Full disclosure: pulpotomy is a very complex procedure with a number of different avenues for performance. I will do my best to describe most accurately the common steps I’ve seen, but understand that the exact actions your dentist or endodontist may take could vary. As with any medical procedure, the first step in treatment is detection. Untreated cavities will likely not be so hard to detect. If inserting an implement into a cavity is able to proceed far enough and ends in a very painful “spike,” it’s likely that a pulpotomy is necessary. Abscesses can be seen in an x-ray, as shown. Additionally, the dentist may massage the gums at the base of the tooth or lightly tap on the crown to test for sensitivity. On the contrary, a traumatized tooth will be tested, either by tapping or extreme cold, to test for a lack of sensitivity, which indicates tooth death. Following a positive test, the dentist will likely talk with you and decide based on finances and your particular circumstance whether extraction or pulpotomy is the best course of action. In the case of a smaller abscess, an antibiotic alone might be enough to quell the infection, however this is not often the preferred treatment.
If a root canal is chosen, the patient will receive either local or full block anesthetic for the corresponding mouth quadrant. The dentist will then drill with a dull drill head down to the pulp chamber and remove the infected pulp with an instrument which resembles a tiny ice cream scoop. If your pulpotomy is due to an untreated cavity, your dentist may skip the next two steps and skip to preservation and sealing. However, if you require the full procedure, next is to remove pulp from the roots of the tooth using small brush-like instruments called files. Once this tissue is removed, the root is cleaned and filled. Modern root canals are usually filled with a heated plastic-like substance which, when dried, fills any cracks or crevices and prevents any further infection.
Once the procedure is completed, the area is once again thoroughly cleaned and sealed. The crown of your tooth will then be prepped for an artificial crown placement. Following your visit, your dentist will most likely prescribe an antibiotic to prevent further infection, so it is absolutely necessary to follow their orders exactly.
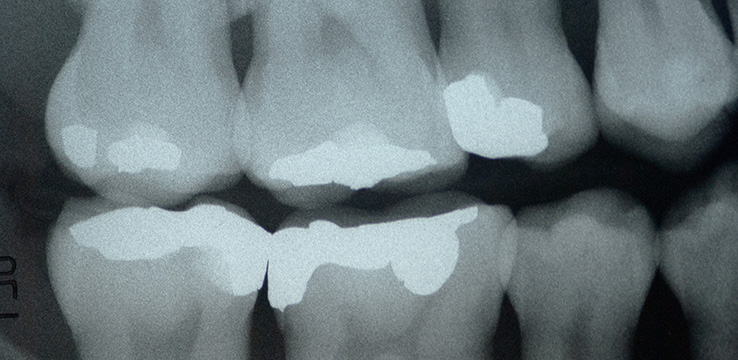
For those who are interested, the roots of a tooth which has undergone a root canal will become radioopaque because of the filling material, as shown below. In all, root canals are not as bad as they are made out to be, and the consequences of evading one are far worse. As always, make sure to take care of your teeth and keep up with regular appointments to maintain optimal health.
In my experience shadowing dentists, it has occurred to me that nobody walking in quite knows the different people working in their mouths. Admittedly, I didn’t know these positions, either, until I began to shadow. We’re taking a break from hard dental science this week to look into just who is walking around in all those funny clothes while you visit the office.
I’ve seen some dental offices with as many as twenty people on staff at one time. There are some offices in bigger cities that boast an even larger payroll, especially in clinic-style offices. However, the smallest office size you will likely ever encounter is four. Within a dental office, there are four essential jobs which must be completed. That isn’t to say only one person can fill each job; on the contrary, most dental offices will have several of one or more of the specialists listed below.
Is There a Doctor in the House?: The Dentist
I know, shocking. A dental office must obviously have a dentist. Almost always, the dentist is the only practitioner in house who is licensed to perform destructive procedures, such as drilling, root canal, and extraction. Most often, a private office will have one to three practicing dentists. In a majority of cases, the office will be owned by one or more of these dentists, however there is the rare exception of an external practice owner.
He or she will have completed a bachelor’s degree in the field of their choosing, so long as they satisfy a laundry list of science prerequisites for dental school. They will either have attained an additional four-year degree called a DDS, Doctor of Dental Surgery, or DMD, Doctor of Medicine in Dentistry. There is no difference between these degrees aside from their name. Both must pass state board exams to be allowed to practice. Your dentist’s classification depends solely on what their school decided to call it.
Just Scratching the Surface: The Dental Hygienist
Your dental hygienist is the person who cleans and examines your teeth during your (hopefully regular) six-month checkups. They will also take x-rays of your teeth and scan for conditions such as abscesses or oral cancer. Although it may seem like the hygienist doesn’t do much, an argument can be made that you’re more so your hygienist’s patient than your dentist’s. In fact, if there aren’t any pressing concerns with the condition of your mouth, the dentist serves as little more than a second set of eyes to check the hygienist’s work and make sure they didn’t miss any concerns. The hygienist acts as the first line of defense in oral care and is integral to any patient’s treatment.
Your hygienist has obtained, at minimum, a bachelor’s degree in dental hygiene and passed their own set of state board exams, similar to your dentist. Some hygienists are beginning to receive certifications beyond their degree, such as the ability to drill teeth, but these certifications are rare as of now.
With the Assist: The Dental Assistant
People often mistake dental assistants for hygienists. Indeed, hygienists are certified to assist, but depending on where you live, you may also be. The easiest way to tell the difference between a hygienist and an assistant is to know that your assistant will almost never be cleaning your teeth beyond rinsing them with water. In most cases, you will only encounter a dental assistant if you’re having work done. As the name implies, the dental assistant’s job is to assist the dentist in his or her procedures. This could mean anything from holding the suction in a patient’s mouth for an hour all the way up to assisting with sutures.
In many places, dental assistants do not need any kind of certification. It is incredibly common for them to have earned a radiography certification, or perhaps to have attended some dental assisting classes. Occasionally, after two years of experience, a dental assistant will apply to become what is called an expanded function dental assistant, which is often shortened to EFDA. This certification allows a dental assistant to fill teeth once the dentist has drilled them, allowing the dentist to focus on other, more complex procedures. EFDAs are somewhat controversial in the field, as some dentists hesitate to put their own name on another person’s work. Regardless, the dental assistant remains an essential part of any dental office.
Putting the Office in Dental Office: The Office Manager
The office manager, once again, performs the duty prescribed by their name: they manage the office. Of the core specialists, the office manager’s job varies the most between offices. Whereas a smaller office may have the office manager as their only front-of-house staff, a much larger office may see their office manager focusing solely on set specific tasks. The duties of the office manager may include, but are not limited to, answering the phone, contacting insurance companies, managing and distributing office schedules, facilitating office communication, and receiving patients. Office managers also maintain the patient records and, in rare cases, may even step in as a dental assistant if one calls off.
Similar to the dental assistant, the office manager does not necessarily require a degree. However, an applicant with a degree in business management or a similar field is often given very high preference.
Finding a Balance: How Staff Size Affects Practice Size and Vice-Versa
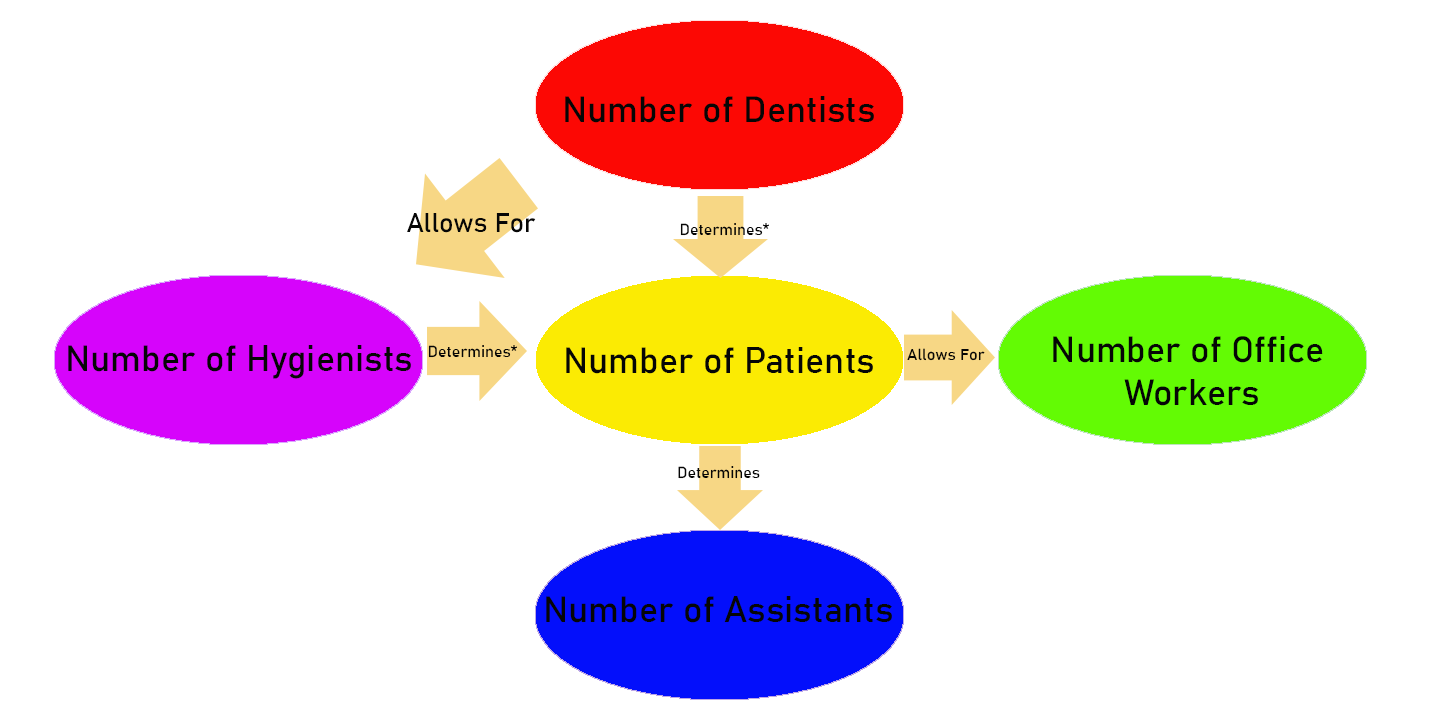
It is worth noting that different practice sizes, or the number of patients attending a practice, will dictate staff size. There are several direct cause-and-effect relationships present within the balance of a dental office. The graphic below shows the most direct relationships, however each of the listed groups affects each of the others in any number of ways.
*Assuming Sufficient Patronage
In all, it takes a small army to run a dental office. Whether it is a small band of four employees or a building full of specialists, no dentist could ever practice alone. Each of the core positions outlined above acts as a part of the backbone of any practice. Each of them is dedicated to making your visit to the dentist as smooth and painful as possible, no matter what procedure you’re having done…unless you live on Skid Row and talk to man-eating plants.
When treating a patient, the dentist’s goal is to administer the most care with the least invasion. He or she will aim to leave as much of the original tooth structure intact and use meticulous, if not graceful techniques to ensure minimal trauma and damage to the mouth. This week, its time to chuck all that froufrou delicacy out the window and yank some teeth! Aright, perhaps this description of tooth extraction is a bit over-the-top, but extraction is known as the most barbaric of the dental practices. As such, it is saved as an absolute last resort in most cases. What can you, as the patient expect if you find yourself on the business end of a set of pliers? We’ll discover that today.
Cuspid’s Last Stand: Circumstances for Tooth Extraction
As mentioned before, extraction is saved for grim circumstances most of the time. Often, patients receiving an extraction will have neglected their teeth to the point that there is no repairing them. When a significant enough portion of a tooth’s structure has been compromised, there are only so many options, extraction being the easiest. Other times, a patient may receive treatment which contributes to the breakdown of tooth structure. For instance, a filling a patient received when they were young may, after several decades, begin to act like a wedge, splitting the tooth beyond what a crown can cover. The third and most tragic circumstance is when a patient’s socioeconomic circumstances or insurance prohibits them from receiving the best care, and extraction is the only practical treatment option for them. We’ll save lamentations about dental insurances for another day, but suffice it to say that it is unfortunately common that a patient who could be an otherwise excellent candidate for advanced treatment is unable to afford it. Extraction may be the only choice.
However, not all reasons for an extraction are so dire. If a patient’s mouth is overcrowded with teeth, it may be advantageous to have some removed. This is the case for many preteens who have a premolar removed before getting braces, for example. Other times, a tooth may simply arrive inside the mouth in a non-sustainable orientation, such as horizontally. The vast majority of the population requires the extraction of their wisdom teeth for one or both of these reasons. As with any branch of healthcare, each patient’s treatment is unique in dentistry, and extraction may be the best option in any number of situations.
Not Quite Music to Your Ears: Instrumentation
The picture above shows the basic instrumentation used in a dental extraction. It is possible that your dentist will have more or less equipment than what is pictured above, but so long as he or she isn’t reaching for fishing line and the doorknob, all is well. Starting from the right, you see basic forceps and a mirror. Skipping to the sixth implement from the right, you see a probe. These are essential for any dental procedure, as they help the dentist see, feel, and work inside the mouth effectively. The three tools in the middle which look like weird ice picks are called elevators. They don’t play smooth jazz unfortunately. Finally, the two instruments on the left are also forceps, except these are meant to grasp teeth instead of cotton squares and swabs. They are shaped slightly different from each other, and your dentist will select the correct forceps based on the shape and placement of the tooth that is to be extracted.
Going Up: The Procedure
As with most dental procedures, the dentist will first numb the region in preparation for extraction. Expect a full block in most cases as opposed to an infiltration, as extractions can otherwise be rather painful. (Refer to last week’s post on cavities if you don’t know what these terms mean). After thoroughly numbing you, the dentist will line the surrounding area with cotton so as to catch any blood which may come from the gums during the course of the procedure.
From there, an extraction is relatively straightforward. As shown in the graphic above, your tooth is held to either the maxillary or mandible via little fibers called ligaments. Ligaments are everywhere in the body and connect bone to more bone. They do a great job of anchoring your teeth firmly in your mouth, but with extraction, that is precisely the opposite of the intended outcome. So, these ligaments must be broken. This is where the elevator comes into play. The elevator’s job is to wedge between the tooth and the jaw bone to loosen the ligaments holding them together. Using a wedge and lever motion on the neck of the tooth, the elevator may also begin moving the tooth away from the jaw. In older or weaker teeth, this may be enough to extract the tooth, alone. Most of the time, however, the tooth will be loose, but not yet extracted at this point.
By the time your dentist reaches for his extraction forceps, find peace in knowing the procedure is nearly complete. The dentist will grasp the tooth with the forceps and gently rock and gyrate the tooth until it fully detaches from the bone. My dentist prefers a “figure eight” sort of motion, but as with most things in dentistry, there is no exact science to it. Having successfully removed the tooth, the dentist and assistant will then check to make sure no root fragments are left behind before cleaning and suturing the wound.
As with last week’s post, I would again like to highlight how helpful nitrous oxide can be in helping calm yourself for what can be a traumatic experience if you have any aversion to the dentist. Again, there is no fear of stigma, and often no fear of cost involved in asking for this treatment. Nitrous exists in a dental office to be used, and can make the entire experience smoother for everyone.
Aftermath: What to Expect
Following your extraction, your dentist will likely prescribe an antibiotic and perhaps a painkiller. Depending on the circumstances, simple over-the-counter pain killers may suffice, but the antibiotic is crucial in making sure the open wound does not cultivate infection. There will be some dull, aching pain involved in the following week, but if the pain ever becomes sharp or excruciating, the blood clot forming under your suture may have dislodged. This is called dry socket.
It is important to visit the dentist if you suspect you may be experiencing a dry socket, as blood clot formation is absolutely necessary in the healing process. Your chances of developing a dry socket increase if you perform a sucking motion or engage in vigorous physical activity. This is why the dentist will suggest not using straws or cigarettes, or perhaps taking an easier day at the gym.
In terms of future care, your dentist may place a bridge to replace the tooth that was extracted, leave the gap as is, or suggest an implant. Next week’s post will cover implants, but for now, it is important to know the difference between proper implants and mini implants. Mini implants are a very niche sort of treatment and, while significantly cheaper than proper implants, are usually a failure in both the short- and long-term. If your dentist suggests a mini implant rather than a proper one, carefully consider receiving a second opinion.
In all, an extraction can be scary to think about. It would be a disservice to say that it is a necessarily pleasant experience, so I won’t. Just know that if you are having a tooth extracted, it is a relatively fast and simple procedure. Afterwards, make sure to follow all of the directions given to you and follow up with the dentist as needed; otherwise, you will regret not doing so. All dental procedures have their time and place. Some aren’t as pretty as others, but taking care of your personal health often means enduring unpleasant experiences from time to time. However, having an extraction is far better than an infected tooth or an overcrowded jaw littered with cavities. So, if you need an extraction, it is best to bite the bullet. Just make sure you bite it carefully, or you may need to have more extractions; bullets aren’t typically chewable.
We’ve all been there. Okay, maybe not all of us, but the vast majority of people have experienced that moment of terror when we hear those words for the first time. “You have a cavity.” Or even worse, cavities. The very thought of it makes one shudder, but what exactly is a cavity, how do you end up with one, and what is the treatment? These are the pressing questions we’ll be answering today.
Into the Thick of It: The Microbiome of Your Mouth
Take just a second out of all this dentistry talk and transport yourself to a rainforest. Imagine the environment. If you’re anything like me, you first notice (and feel compelled to point out) how goshdarn humid it is. Or, if that’s just my midwestern upbringing speaking, the first thing you notice might be the vast variety of species around you. The rainforest is home to millions of unique species, many of which are not found anywhere else in the world. Each plays a critical and unique role in their biological community, called a biome. There are a handful of specific biomes in the natural world, all characterized by the climate and species one can expect to find in them.
So, why discuss biomes when talking about human health? Every pre-health undergrad asks themselves this at some point, because we all have to learn it. In this specific context, it’s important to understand what a biome is so that we can effectively establish the human body as one. Your body is perhaps one of the most complex ecosystems in the known world, but it’s still a biome. It is defined by its own niche climate and species, which is unique to even another person’s.
The mouth is what we consider a microbiome. A microbiome is a region within a biome which is distinct from its surroundings. It is not isolated enough to be considered sovereign, but is unique enough within the context of a single biome to be singled out. Think of a snowy mountaintop in a deciduous forest, or an oasis within a desert. Your mouth is a microbiome which is home to as many as several billion bacteria. It is warm and also goshdarn humid, making it very similar in variety and in climate to the rain forest we mentioned earlier. Your bacterial flora, meaning the bacterial variety and makeup, is unique to any other person’s and changes based on diet, oral hygiene, and other external contact. I’m sorry if I’ve ruined kissing for you forever, but what’s more intimate than exchanging oral bacterial flora? I can’t think of anything.
Cavity: An Origin Story
Most people were taught at a young age that plaque is bad, but seemingly nobody knows what it is. Perhaps that is for the better, but today, we lift the veil. Bacteria feed on the billions of food and beverage particles leftover in the mouth after we eat and drink. One of the fundamental laws of biology is this: that which consumes must also produce waste. In the mouth, we call this microscopic manure “plaque.” However, instead of telling you that your teeth are covered in bacterial boom-boom, your dentist likely notes the buildup of plaque on the tooth surface and advises you to brush and floss more. This may sound nicer, but I believe the first approach may be more effective. If you’re anything like me, the idea of a billion little microorganisms pooping all over your teeth is pretty compelling. I sincerely hope that isn’t just my midwestern upbringing speaking.
Unlike our own feces, our oral flora uses their waste to anchor themselves to the teeth, where they are most likely to receive even more nutrients and release even more dental dung (seriously, brush your teeth). Like our own feces, that of your oral flora can vary in composition depending on their diet. Some foods, most notably the infamous sugar, acidifies the waste. It’s common knowledge that acid degrades organic material, of which our teeth are made. This acid number two, in other words, eats away at enamel, causing pits in the teeth. These pits are called dental caries, or cavities.
Pits of Despair: Detection and Treatment
A bite wing x-ray showing a very obvious dental cary.
Cavities aren’t always able to be seen by the naked eye. Often, there is discoloration, sensitivity, or a visual deformity in a tooth that gives away the presence and location of a cavity, but the most common way your dentist can tell whether or not you have one is by viewing an x-ray, like the one shown above. Teeth are relatively radio-opaque, meaning they show up mostly white on an x-ray. A cary, as you can see, will show in an x-ray as a region of lesser radio-opacity. The dentist or hygienist who views your x-ray may probe around with one of their instruments to verify what they have seen. They will then speak with you about receiving a restoration, or filling.
A restoration procedure consists of three steps: drilling, prepping, and filling. Before beginning the procedure, the dentist will usually administer anesthetic. If the shot is administered to the very back of your mouth, it is called an alveolar block, or “block” for short. This will numb an entire quadrant of the gums, tongue, and lips, and is used when filling the molars or when more than one tooth is to be filled within the same quadrant. If the shot is administered anywhere else in the gums, it is called infiltration. This numbing will be more specific, but less effective, and so is used more toward the front of the mouth than toward the back. Once the anesthetic sets in, the restoration can begin.
First, your dentist (or, in rare cases, a heavily-licensed hygienist) will carefully drill the tooth that is in need of filling. The aim will be to maintain as much of the tooth’s original structure as possible while also ensuring that all of the decaying portion is fully removed. Next, either the dentist or an EFDA (expanded function dental assistant), who is certified to fill teeth, will prep the tooth to be filled. This includes disinfecting the tooth with a special tooth shampoo, rinsing, and lining the pit with an abrasive surface with adhesive. Finally, the actual “filling” can begin. There are two kinds of filling: Amalgam and composite. Amalgam is the “old school” approach to filling and was previously the predominant filling material. If you have a “silver” filling, you have amalgam. Composite is a white ceramic-like substance that is generally more popular because it can be produced in a number of different shades to match that of a tooth. Additionally, new composite materials are being produced which can rival the strength of amalgam. Both materials work well for filling a tooth, however, and your dentist may choose to use either depending on the circumstances. Once filled, a composite filling must be cured with a bright blue light. After some quick sanding of the new restoration for comfort, your filling is complete! For those who are curious, fillings are entirely radio-opaque, as shown in the picture below.
As a brief aside, the thought of receiving a filling terrifies some people, and there is nothing wrong with being afraid. Most modern offices offer nitrous oxide to their patients, often for free. This gas usually comes through a mask which is placed on the face and merely serves to take the edge off of this sort of anxiety. You should feel no shame in asking for this treatment, as I have even talked to some dentists and hygienists who prefer to use it, themselves, sometimes even for their regular cleanings. It is harmless and makes the experience less traumatizing for you. The dentist will also have an easier time working on a less tense patient. Restorations are a relatively easy and well-practiced procedure, but the concern for mistakes increases if the patient feels scared or uncomfortable.
Cavity Prevention for Dummies
In all, nobody wants to have a filling. The best way to make sure you don’t end up needing this procedure is simply to take care of your teeth. Brush twice daily to free your teeth of all that recycled refuse we call plaque, but also make sure you floss once a day. A very large portion of restorations are performed on the distal or mesial surfaces (see my previous post if you don’t know those words) because people fail to remove the plaque between their teeth. The easiest solution to this problem is to floss once daily. Otherwise, maintain regular appointments with your dentist so that if you do end up carrying a cary, you can carry out treatment as soon as possible. If left to expand to the pulp, a simple cavity could lead to a root canal, or even tooth removal. Often, by the time you are able to see or feel a cavity, it is already too late. Brushing and flossing prevent a majority of cavities, but not all cavities can be prevented. Allow your dentist to detect them early, lest you end up much worse off in the future.
There are so many things to know and discuss in terms of taking care of your mouth. What better way to begin than introducing the structures within the oral cavity? Think of this as taking a tour of your own mouth except you won’t ruin your shoes! In all seriousness, it is much easier to understand the complexities of oral health if you first have a basic understanding of the road map.
The oral cavity is the very beginning of what is called the alimentary canal, a fancy-sounding term for digestive tract. The alimentary canal sees nutrients enter through the mouth, pictured above, and solid waste leave through the anus, thankfully not pictured anywhere, and includes your esophagus, stomach, and the small and large intestines in between. The focus of dentistry is kept mostly to the first two stops, the mouth and esophagus. Looking in the mouth, one can see that there are three distinctive sections, being the teeth, which are bone-like, the tongue, one of the most powerful muscles in the body, and all the other fleshy pink “stuff.” This “stuff” is called mucosa, and it lines the entirety of the alimentary canal. The mucosa is soft and malleable, yet very thick and resistant to damage, thanks to its many cell layers. This mucosa lines several important structures in the mouth, most notably the gingiva, or gums. Also covered by mucosa are the floor of the mouth, which contains salivary glands, the buccal region, so named because it shields the buccinator (cheek) muscle, the tonsils, which play a minute role in the immune system, the uvula, which helps prevent milk coming out your nose every time you drink it, and the roof of the mouth, broken into the hard and soft palate. The hard palate is simply your maxillary bone, in which your maxillary (upper) teeth are rooted, fused with the palatine bone toward the back. If you move your tongue back along the center of the hard palate you will feel a sudden depression called the soft palate, which is where the palatine bone ends. The soft palate ends in the oropharynx, the back of the throat, which leads to the esophagus and the trachea so you can eat, drink, and breathe properly.
Something to Chew On: The Teeth
The oral cavity is extremely complex after a closer look. However, “dentistry” comes from the Latin dent, which means, unsurprisingly enough, “tooth.” Indeed, dentists are most concerned with teeth. As mentioned before, the maxillary teeth fit into the maxillary bone, and the logic follows that the mandibular (lower) teeth are rooted in the mandible, or jawbone. Shown above are four different ways that the teeth are identified. Many people have tried to reinvent the tooth identification wheel, but the quickest to learn is the universal method, shown in purple. This is the system most dentists use in office shorthand, and is the system to which this page will refer at all times. To figure it out, simply place your tongue on your third molar, or wisdom tooth. If you have had your wisdom teeth removed or if they haven’t come in yet, you still count as if the tooth were there. (If you haven’t had your wisdom teeth removed, stop reading now and schedule a consultation with an oral surgeon just in case.) This upper right wisdom tooth, or corresponding void, is number one. Keep counting tooth by tooth until you reach eight, remembering to count gaps for any teeth you’ve had removed. You should have reached your right front tooth. Congratulations! You’ve counted your upper right quadrant. Continue moving leftward, counting your maxillary teeth until you reach sixteen. Then, turn the corner and drop directly to the lower left wisdom tooth, which is tooth seventeen. Proceed from the left all the way to the lower right wisdom tooth and you should reach thirty-two.
Now that you can identify all the teeth in your mouth by number, let’s return to the first eight. You will notice that each quadrant normally contains the same teeth as the others, so by observing this first quadrant, we can extrapolate for the other three. Within this quadrant are three or four distinct zones. The first, teeth eight, seven, and six, make up the anterior region. These are the teeth you use to smile at your loved ones, and also the ones you use to rip and tear food to shreds. Quite the bait-and-switch for that poor apple you just ate, eh? Teeth eight and seven are called incisors (think in-scissors, because they cut up your food), while six is called the canine because the same tooth is enlarged for use in holding onto prey in predators such as dogs. Because the structure of the canine is slightly different from the incisors and drastically different from the next group, people often give them their own classification, whilst others believe that makes them too conceited. Imagine giving Kanye his own zip code. Regardless, the canine’s neighbors to the back are called premolars. The premolars, teeth five and four, are facilitators. They help continue to cut up food and start the grinding process. But this isn’t sophomore homecoming. Grinding in this context is vital and makes it easier to digest large chunks of food (the other just makes things harder). This is where teeth three, two, and (maybe) one shine. These teeth, called the molars, are flat and broad. They help crush and mash up food for continuation through the alimentary canal. Unlike the other teeth, the molars don’t have a “baby” equivalent. Three, two, and one normally grow in around ages six, twelve, and eighteen, respectively. They are extremely developed in herbivores, as rough grass and plants need extra processing before digestion. They are just as important in humans as incisors, as we are omnivores. In fact, archaeologists are able to determine whether ancient species were herbivorous, carnivorous, or omnivorous based on which teeth in their skulls are most developed.
Digging Deeper: Tooth Anatomy
Finally, we zoom in for a closeup of the innerworkings of an individual tooth. To the left of the graphic above, we see the three distinct regions on a tooth. The crown is what most people consider when they think of their teeth. It is the region we see when we smile and the part we (should) brush and floss every day. The crown is further broken down into five surfaces for office shorthand. No matter the tooth’s position in the mouth, the surface facing toward the midline is called the mesial surface and the one facing away is called the distal. The lingual surface is called such because it’s in contact with the tongue, and the buccal surface because it maintains contact with the buccal mucosa (remember, that’s your inner cheek). Finally, the occlusal surface is the biting surface, or the surface that touches other teeth when you “oc-close” your mouth. Moving downward, the neck is the portion of the tooth where the crown meets the gingiva, which quickly transitions into the root. The root anchors the tooth firmly into bone, either the maxillary or mandible from before. The root is arguably the most important part of the tooth, as it connects the tooth to the rest of the body via nerve and vessel canals in the sensitive pulp of the tooth. Another name for a root canal is a pulpotomy, which translates from Latin into “removal of pulp.” The pulp is surrounded by a spongy tissue called dentin, which is fragile connective tissue that must be protected by enamel. Enamel is the strongest substance in your entire body, which is absolutely necessary for the amount of attrition (physical stress), erosion (chemical stress), and decay (bacterial stress) it can face. Enamel is vitally important to maintain, as it can never be naturally replaced, but is absolutely invaluable in maintaining tooth integrity.
There are many aspects of the oral cavity that are vital to maintain good dental, as well as overall health. Enamel is perhaps the most important, but indeed all of the complicated ins and outs of the mouth are crucial to maintain. Luckily, dentists and their staff invest years of education and training (and a small fortune) into learning how to help you take care of your oral health. That is why it is imperative to schedule regular dentist visits and maintain your oral hygiene. Brush twice and floss once daily, but let the professionals do the rest. You and your smile will be better for it.
Breaking the fourth wall to briefly introduce myself
My brother, Cory (Left) and I (Right) at a leadership conference in Marietta, Ohio
Before I write anything about how to take care of your smile, I first felt the need to introduce myself and explain a little about my background. My name is Ryan Burkhart. I am entering my fifth year pursuing a degree in chemistry at Muskingum University, a small liberal arts college in New Concord, Ohio. I am currently applying to dental school and, as such, have spent many hours shadowing dentists. I believe this puts me in the perfect position to write this sort of blog. While I know and understand, at least to a certain extent, many of the day-to-day operations of a dentist, the world of dental health is still fresh and new enough to me that I can more easily describe things in an understandable way. At the same time, I will be researching and solidifying topics that will be important for me to know in the future. If I can have some small influence on oral health awareness while better preparing myself for my future, I will consider this venture a success. Thanks for reading and helping me to achieve my goal!